In this article, I share the results of an assessment study designed to provide an adapted aquatics and rehabilitation class, feedback on successful areas of instruction and areas that may need improvement. Although several adapted aquatic swimming assessments exist (e.g. Special Olympics, DePaepe Checklist, Sherrill Model) only the Conatser Adapted Aquatics Swimming Screening Test is norm-based and allows statistical analysis.
This assessment has 44 total test items consisting of (a) psychological/physical adjustment skills, (b) entering and exiting the pool skills, (c) acceptance towards passive range of motion, (d) breath control and respiratory skills, (e) balance and flotation skills, and (f) swimming movement skills through the water. Pre- and post-aquatics skills of children with disabilities were assessed by trained university students. These students also conducted the instructional intervention.

A screening test was used to establish a baseline of essential swimming skills to be taught in the adapted aquatics programs. Before testing and instruction, the university students were trained for one week on how to conduct the assessment and learned techniques for teaching swimming to children with disabilities. Children with disabilities received instruction for 3 weeks, Monday through Friday, with each session lasting 1 hour. Pretest assessment guided instruction and the acquisition of new skills. Instructors used a variety of motivating incentives (e.g. equipment, encouragement, musical, games etc.) to improve swimming performance. An emphasis of instruction for children with disabilities was to ensure they learned how to be safe in and around the water environment.
A total of 41 children and young adults, 30 males and 11 females, between the ages of 3 to 22 were assessed (Mean ± STDEV age = 9.43 ± 0.69). Children’s disabilities included intellectual (ID), autism, cerebral palsy (CP), spinal cord injury (SCI), visual impairment (VI), traumatic brain injury (TBI) and attention deficit hyperactivity disorder (ADHD). Assistance was provided depending on their ability and severity. For example, children that used a wheelchair were manually lifted in and out of the pool, used a life jacket, and had two instructors. High ability children were placed in small groups (2-3), with one instructor who could choose whether or not to use flotation devices such as life jackets, noodles, and kick-boards. All instructors developed an individual and unique plan for each child with a disability, taking into consideration the child’s interest, family input, and the results of the swimming screening assessment. Instructors laminated (waterproofed) their intervention plan(s) and kept them pool-side for quick reference.
The results of our assessment and the subsequent interventions are illustrated in Figure 1
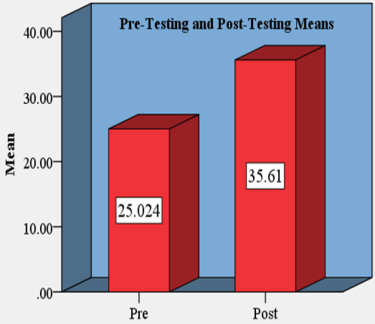
Figure 1. Changes in means from Pre-Testing to Post-Testing scores. Pre- testing scores were obtained within the first 2 days and post- testing scores were obtained on the last day of the program.
Figure 2 shows the distribution of the various types of disabilities:
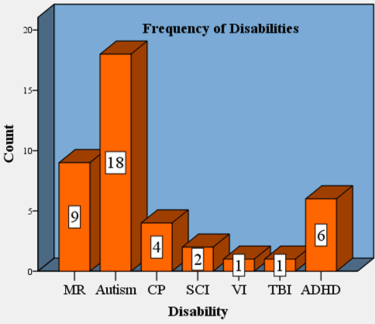
Figure 2. Distribution of Disabilities. Shown are the count of individuals with disabilities who participated in the adapted aquatic program.
Data analysis was conducted using the IBM SPSS version 23 statistical package. T-test results showed a highly significant difference (p <0.01) between the pre- testing and post- testing assessments. Pre-test assessment had a mean of 25.0 with an STDEV of 1.7 and a post-test assessment had a mean of 35.6 with an STDEV of 1.2. Children with disabilities improved from an initial 56% completion of the assessment test to a subsequent 80% completion. In other words, the swimmers showed an overall improvement of 10 aquatic skills: Evidence that our adapted aquatics and rehabilitation program was successful.

Our hope is that the skills gained will help these children and young adults with disabilities become better swimmers, safer, and more mobile in the water. Anecdotal observation by parent and students observed an increase in land-based activities (balance, walking, up/down steps, wheelchair mobility, posture, etc.), verbal communication, and a general overall increase in health/fitness.
Summary
Successes Observed
– Using pre-assessment to guided instruction
– Having a fun-play style format, with lots of games, and music
– Having a one or two to one ratio and small group instruction
– Using lots of equipment (balls, kick-boards, noodles, flippers, masks, diving sticks, standing platforms, etc.,)
– Daily focusing on different ways and strategies to teach assessment skills.

Improvement Recommendations
– Instruction focused on (e) balance and flotation and (f) active movement in the water. Although children increased on average 10 skills, these two areas had the lowest improvement.
– Increase adherence to the program. The program started with a total of 57 children and ended with 41 children. Strategies to encourage and promote participation need to be considered such as calling parents after absentees, daily giveaways, and perhaps gas vouchers.
– Increase equipment access and availability. Equipment was not stored on-sight and had to be carried in every day by several students. If the student-instructor was late or missed class equipment was unavailable. This interfered with instruction and children’s on-task time.
– Longer preparation and training university students on how to assess and instruct children with disabilities in adapted aquatics. We only had one week to prepare students thus, need better use of class time and move from 1 to 2 days of training in the pool.
– Longer instructional sessions for the children. One hour is not enough for children with disabilities to get in the pool and on-task. A 90-minute class would allow for all transitional needs and preparation factors, thus hopefully achieving a full 60-minutes of learning swimming skills.
– Move from 3-weeks to 4-weeks of adapted aquatics. Because most of the children in swim programs like this have severe disabilities, it takes lots of practice for them to learn new skills. This is probably the only swimming opportunity offered to them for the summer. High functioning disabilities can usually “blend” into “normal” summer swim programs with little to no modifications, however severe disabilities require modifications (instruction, variations in equipment, better instructor-to-children ratios) and are often not readily available.

I hope the suggestions I’ve shared for improving my adapted aquatic program will help you improve yours. I encourage the use of assessment-guided instruction and some simple statistically guided analysis with pre- and post-testing to truly see whether your instruction is making a “significant” difference.
